
Blepharoptosis is the drooping of the upper eyelid. Unilateral ptosis is common, but drooping of the eyelids on both sides is possible. Ptosis of the upper eyelid of one eye of 1.5 – 2.0 mm, as a rule, leads to asymmetry in the position of the eyelids and represents a cosmetic problem. With severe ptosis, the eyelid closes the pupil, which leads to visual impairment: limited field of vision, difficulty in reading, and even the inability to see without lifting the upper eyelid with a hand.
Causes of Blepharoptosis:
The drooping of the upper eyelid may appear with age or after eye operations (cataract extraction, antiglaucomatous, vitreoretinal interventions, etc.).
In this case, the tendon of the muscle that lifts the upper eyelid is lengthened, or its partial detachment occurs. One type of ptosis caused by impaired innervation of the smooth muscle of the upper eyelid is partial ptosis in Horner’s syndrome. Acquired ptosis also occurs due to trauma, inflammation, tumors, intracranial aneurysms, and other causes. With paralysis of the oculomotor nerve, the drooping of the upper eyelid is usually unilateral complete and is combined with a violation of the mobility of the eyeball. In a severe autoimmune disease, myasthenia gravis, bilateral (usually asymmetric) drooping of the eyelids often occurs. Often this pathology is combined with binocular double vision and nystagmoid movements of the eyeball.
Kinds of Blepharoptosis:
The classification of ptosis of the eyelids involves the allocation of the following forms:
• congenital, which is present in a child immediately after birth or can be determined during the first year of life;
• acquired – appears in a person as a result of eye diseases, pathologies of the nervous system or is a consequence of facial injuries, as well as aging.
By localization, Blepharoptosis is divided into unilateral and bilateral.
Doctors also distinguish 3 degrees of Eyelid Ptosis:
• First degree. The lowered eyelid covers only 1/3 of the pupil.
• Second degree. The edge of the eyelid covers ½ of the pupil.
• Third degree. The pupillary opening is completely closed by the overhanging eyelid. On the side of the lesion, the eye cannot see completely due to a mechanical obstruction.
Diagnostics:
If eyelid ptosis is suspected, the diagnostic program may include the following methods:

• visual examination by an ophthalmologist;
• determination of the width of the palpebral fissure – this is the distance between the edge of the upper and lower eyelids, measured in a calm state;
• definition of MRD is the distance from the edge of the upper eyelid to the central part of the pupillary opening;
• visometry – determination of visual acuity;
• tonometry – measurement of intraocular media pressure;
• ophthalmoscopy, which allows to assess the condition of the fundus, tear film, cornea;
• ultrasound scanning of the eyeball and adnexa;
• magnetic resonance imaging of the brain with contrast (to assess blood flow and exclude cerebral problems);
• computed tomography of the orbits.
The diagnostic program is aimed not only at assessing the degree of ptosis, but also at identifying the possible causes of this condition.
In order to correct the position of the upper eyelid, the following methods of surgical treatment are used:
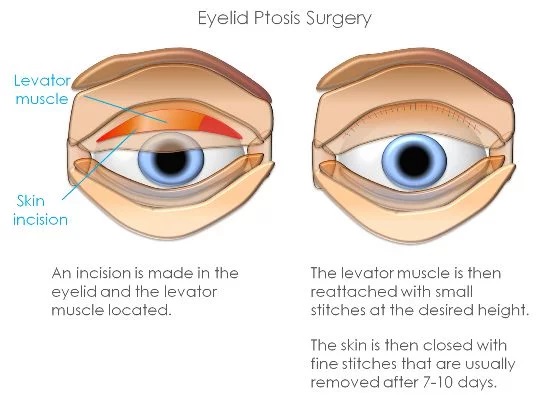
1. Operations on the muscle that lifts the upper eyelid
• resection of the aponeurosis and muscle body
• translocation of the tendon part, the muscle that lifts the upper eyelid, and its fixation to the tarsal plate or the formation of its duplication, followed by fixation of the latter to the tarsal plate of the eyelid.
2. Resection of the superior tarsal muscle (mullerectomy operation)
3. In severe cases, with low mobility of the upper eyelid, operations of a “suspending” type are performed, during which, with the help of special materials, a connection is made between the eyelid and the frontal muscle.
These techniques involve a thorough examination of the patient, in particular the conduct of special tests before surgery. The patient is instilled with a solution of phenylephrine (causes stimulation of the receptors of the upper eyelid), which leads to the lifting of the upper eyelid. In this case, the patient is given the opportunity to look in the mirror and evaluate the test result. The patient decides whether this position of the upper eyelids suits him. During the operation of resection of the superior tarsal muscle, in 95-98% of cases, this level (previously agreed with the patient) is achieved.
Rehabilitation:
Within 1-1.5 weeks after plastic surgery, swelling of the tissues is noted, which then disappears on its own. The final result of the plasty is evaluated in 2-3 weeks, when the first wave of regeneration ends.
At the stage of rehabilitation, until the tissues are completely healed, it is recommended to regularly change dressings, limit facial movements and wear sunglasses on the street.
To improve the aesthetic result, some patients may be recommended cosmetic procedures, in particular the introduction of hyaluronic acid to create facial symmetry.

Benefits of choosing AstraMedicaGroup
Only top qualified doctors
JCI certificated hospitals
Free COVID-19 Test before departure
4 nights in a 5-star hotel in Istanbul
Costs for laboratory, medication and equipment
Pre/post-operative tests
Free Istanbul tours
Latest technologies
Excelent travel assistance
All-round VIP transfer
Credit / Debit cards accepted
No prepayment
Personal assistants speak in English
24/7 customer service